Western States Overdose Death Data in 2025
Western States Overdose Death Data in 2025 If you work in public health, policy, or harm reduction, western states overdose death data is not an abstract…
Western States Overdose Death Data in 2025
If you work in public health, policy, or harm reduction, western states overdose death data is not an abstract trend. It tells you where the response is working, where it is failing, and where people are still dying before help reaches them. That matters now because the West is not moving in one direction. Some places have started to see declines, while others are still dealing with fentanyl, methamphetamine, and unstable treatment access at the same time. What looks like progress in one state can hide real pain in the next county over.
Look closely and the pattern is messy. That is the point.
What the western states overdose death data is showing
- Fentanyl still drives most fatal overdoses across much of the West, even where totals have started to ease.
- Stimulants matter more than many officials admit, especially in places where meth and fentanyl are showing up together.
- State averages can hide local spikes, so county-level data often tells a more honest story.
- Access to naloxone and treatment remains uneven, especially in rural areas and tribal communities.
- Policy changes do not move death data overnight. The lag is real, and it can be brutal.
Why the western states overdose death data matters to you
If you are trying to plan outreach, funding, or clinic capacity, you need more than national headlines. Western states overdose death data helps you see where pressure is building, where it has eased, and where services are still too thin. Without that, you end up pouring resources into the loudest problem instead of the deadliest one.
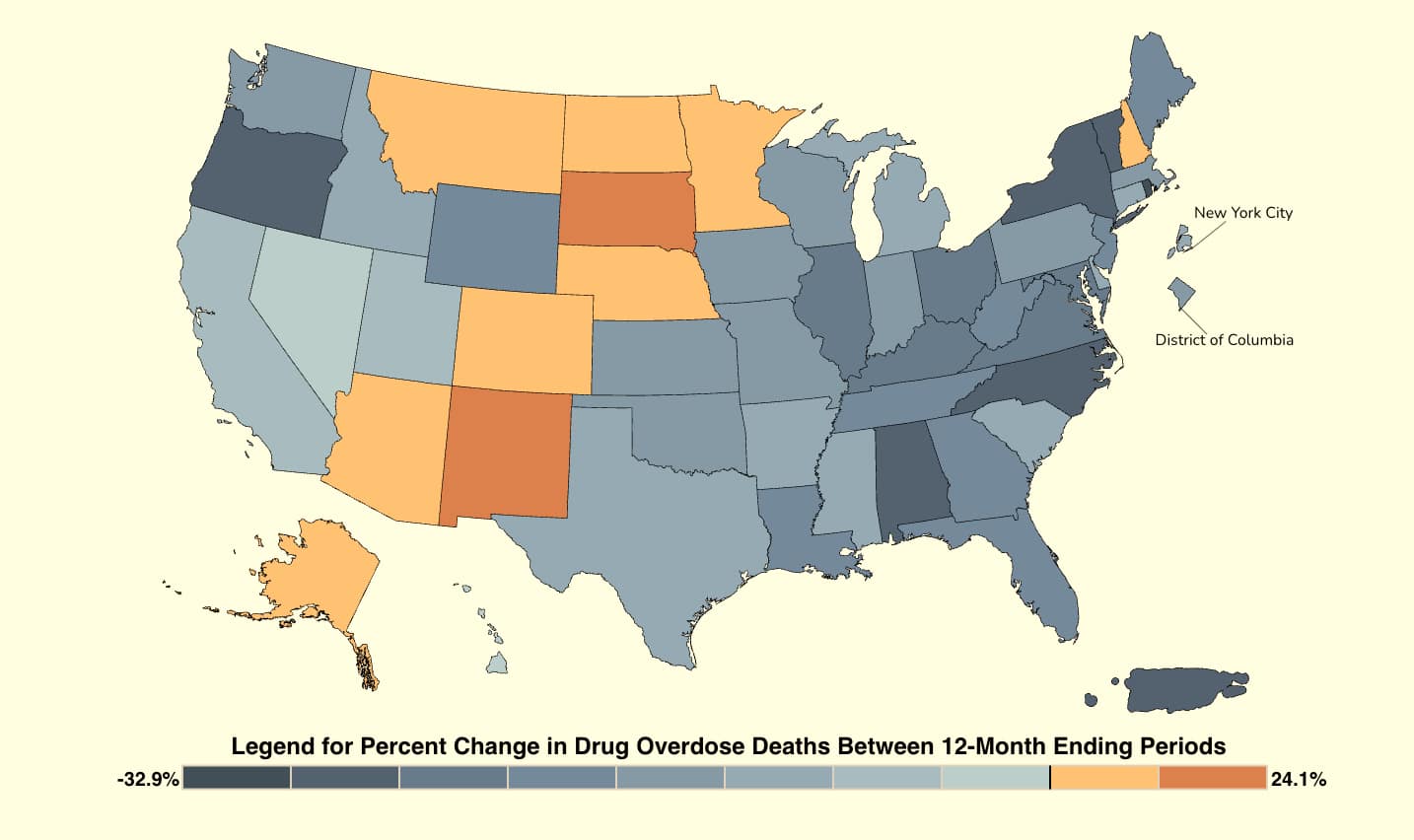
And yes, the regional picture is uneven because the West is uneven. California, Oregon, Washington, Nevada, Arizona, Colorado, New Mexico, Utah, Idaho, Montana, Wyoming, Alaska, and Hawaii all face different drug supply patterns and different policy choices. A county with strong syringe service access may look very different from a neighboring one with few treatment slots and long EMS response times.
One state can post a better headline while a smaller city still cannot get naloxone into enough hands. That gap is where deaths keep happening.
How to read western states overdose death data without getting fooled
Data on overdose deaths can be useful, but only if you read it with caution. Death certificates lag. Coroner and medical examiner practices vary. Some places classify deaths faster than others, which makes a recent drop look cleaner than it really is.
Here is the thing. A year-over-year decline is good news only if it holds after the reporting backlog clears. Otherwise, you are looking at a timing issue, not a durable trend.
Start with the right questions
- Are deaths falling statewide, or only in a few metro areas?
- Is fentanyl still the main driver, or are stimulants rising too?
- Are Black, Latino, Indigenous, or rural communities carrying a larger share of the harm?
- Did treatment access change before the numbers changed?
- Are you comparing provisional data with finalized data?
A good analyst treats overdose data like a kitchen thermometer. You do not guess whether the roast is done. You check the center, not the outside. Same idea here. The surface numbers can look fine while the middle is still undercooked.
Western states overdose death data and the policy trap
Too many officials read any small decline as proof that the crisis is under control. That is wishful thinking. A short dip can come from supply shifts, changing reporting, or local enforcement patterns, not just from better care.
Real progress usually shows up in several places at once. More naloxone in circulation. Faster connection to medications for opioid use disorder. Better response in jails, shelters, and emergency departments. Fewer people falling through the gaps after a nonfatal overdose. If only one piece moves, the whole system is still fragile.
And that fragility shows up fast in rural western states. Long drives to care. Thin EMS coverage. Few detox beds. No backup when one clinic closes. That is not a side note. It is the story.
What the data should push leaders to do next
Western states do not need more press releases. They need boring, repeatable work that reaches people before the next overdose call. That means the same basics, done better and at scale.
- Expand naloxone access through libraries, shelters, schools, pharmacies, and mobile teams.
- Make medications for opioid use disorder easier to start in emergency rooms, jails, and primary care.
- Track stimulant-involved deaths separately so meth and cocaine trends do not get buried.
- Use local dashboards so counties and tribes can act on current data, not stale summaries.
- Fund peer outreach where people already use drugs, sleep outside, or cycle through the justice system.
Honestly, this is not glamorous work. But neither is counting the dead.
What you should watch next in western states overdose death data
The next round of western states overdose death data will matter most if it answers one question. Are fewer people dying because the response got stronger, or because the market shifted again? That difference matters for every budget line, every clinic hire, and every outreach plan.
If you follow this issue, watch for county-level detail, stimulant trends, and changes in access to treatment after overdose. Those are the signals that tell you whether a state is solving the problem or just getting better at describing it. And if officials only talk about statewide averages, ask the harder question. Who is still missing from the picture?
This article is for educational purposes only and should not be considered medical advice. Always consult a qualified healthcare provider before making decisions about addiction treatment. If you or someone you know is in crisis, call SAMHSA's National Helpline: 1-800-662-4357 (free, confidential, 24/7).