Mirtazapine for Methamphetamine Use Disorder
Mirtazapine for Methamphetamine Use Disorder If you are looking for a medication that helps with methamphetamine use disorder, the list is still painfully…
Mirtazapine for Methamphetamine Use Disorder
If you are looking for a medication that helps with methamphetamine use disorder, the list is still painfully short. That gap matters because stimulant-related deaths keep rising, and many people need more than counseling alone. Mirtazapine for methamphetamine use disorder gets attention because it is cheap, familiar to clinicians, and already used for depression and sleep. But does the evidence actually hold up?
Here is the thing. One positive signal can turn into a lot of hype, fast. That is especially true in addiction medicine, where good options are scarce and every promising study gets amplified. The real question is not whether mirtazapine sounds plausible. The question is whether the data are solid enough to change practice right now, and for which patients that answer might be yes.
What stands out
- Mirtazapine has shown some benefit in trials, but the effect size looks modest and the evidence base is still thin.
- The most cited data come from studies in men and transgender women who have sex with men, which limits how broadly you can apply the results.
- Medication is not a stand-alone fix. Behavioral treatment and harm reduction still do most of the heavy lifting.
- Sleep, appetite, and depression symptoms may improve with mirtazapine, which can matter even if methamphetamine use does not fall dramatically.
Why mirtazapine for methamphetamine use disorder is getting attention
Methamphetamine use disorder has been a graveyard for medication trials. Plenty of agents have looked promising on paper, then fizzled in real studies. So when mirtazapine posts even a decent result, people notice.
Mirtazapine is an antidepressant with effects on norepinephrine and serotonin. Clinicians also know it for sedation and appetite stimulation. That profile makes it interesting for people using methamphetamine, who often struggle with insomnia, weight loss, low mood, and chaotic daily rhythms.
But plausible is not the same as proven.
Think of it like a backup quarterback who has one strong game. You pay attention. You do not hand him a long contract after one Sunday.
The trial data on mirtazapine for methamphetamine use disorder
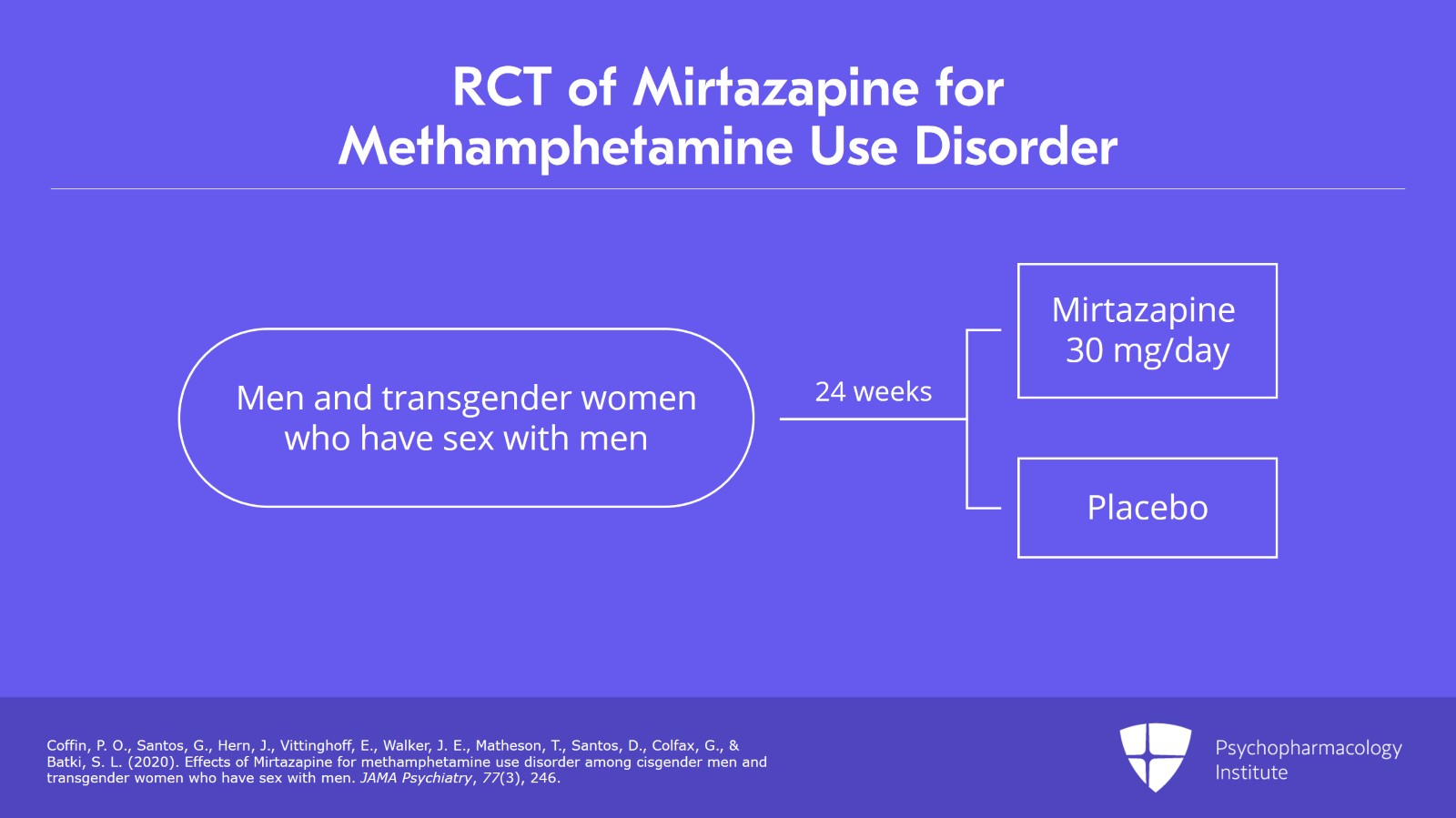
The source article reviews the better-known randomized trial data, especially work led by Colfax and Coffin. In those studies, mirtazapine was linked to reductions in methamphetamine-positive urine tests compared with placebo, alongside counseling.
That matters. It means this is not pure speculation or anecdote.
But the details matter more than the headline. The studies were relatively small. The populations were specific, mainly men and transgender women who have sex with men. And adherence is always a live issue in real-world addiction treatment, where taking a nightly medication consistently can be harder than it looks in a trial protocol.
Small positive trials are useful. They are not the same as a settled answer.
The article’s skeptical tone is justified. A positive signal should push us toward more testing, not toward overstating what we know. If you are trying to decide whether this is standard of care, the answer is still no.
What the studies suggest
- Mirtazapine may reduce methamphetamine use in some patients.
- It may be especially relevant when depression, insomnia, or low appetite are part of the picture.
- The evidence does not support presenting it as a reliable medication solution for all patients with stimulant use disorder.
Who might be a reasonable candidate?
If I were covering this for a newsroom audience and talking to front-line clinicians, I would frame mirtazapine as a selective option, not a broad recommendation. It makes the most sense when a patient has methamphetamine use disorder plus symptoms mirtazapine can also target, such as poor sleep or depressive symptoms.
That overlap is clinically useful. Sometimes one medication can help with several problems at once, and that can improve engagement.
Still, you need to be honest about the limits. A patient asking, “Will this stop my meth use?” deserves a plain answer: maybe a little, maybe not, and we cannot promise much from the current evidence.
What are the downsides?
Mirtazapine is not a benign candy pill. Sedation can be useful at night, but it can also leave people groggy. Weight gain and increased appetite may help some patients and bother others. And like any psychiatric medication, it can be stopped early if the patient feels flat, foggy, or simply unconvinced it is doing anything.
There is also the larger risk of distraction. If a clinic starts talking about mirtazapine as though it solved stimulant addiction, attention can drift away from interventions that matter more, including contingency management, counseling, safer use support, HIV prevention, and overdose education where fentanyl contamination is a concern.
That drift is a mistake.
How this fits with real treatment for stimulant use disorder
Look, methamphetamine use disorder rarely responds to a single move. Care usually works more like layered architecture than a magic switch. You need a stable frame first, then you add supports that make the structure hold.
For many patients, that means:
- Contingency management when available
- Cognitive behavioral therapy or other structured counseling
- Sleep, nutrition, and mental health support
- Harm reduction services, including safer use education
- Screening for HIV, hepatitis C, and other related health issues
In that setup, mirtazapine may have a role. But it is a support beam, not the whole building (and some buildings do fine without it).
What the evidence does and does not let you say
You can say mirtazapine has some evidence of benefit for methamphetamine use disorder. You can say it may be worth considering for selected patients, especially when insomnia or depression are part of the case. You can also say the medication is widely available and familiar to prescribers.
You should not say it is clearly effective across broad patient groups. You should not imply the evidence is strong enough to settle the question. And you should not skip over the fact that the trial populations were narrow.
Honestly, this is where addiction treatment writing often goes off the rails. A modest study result gets treated like a breakthrough because the unmet need is so severe. The need is real. The leap in language is still a leap.
Practical takeaway for clinicians and families
If you are a clinician, think of mirtazapine as an option to discuss, not a script to reflexively write. Match it to the patient in front of you. Ask whether sleep, appetite, mood, and treatment engagement could improve enough to make it worthwhile.
If you are a family member or patient, ask a sharper question than “Does this work?” Ask, “What problem is this supposed to help first, and how will we know if it is helping within a few weeks?” That question usually gets you a more honest answer.
Where this goes next
The field needs bigger trials, more diverse patient populations, and real-world data that reflect how people actually live, miss doses, combine substances, and move in and out of treatment. Until then, mirtazapine for methamphetamine use disorder sits in the maybe column. Promising enough to keep studying. Thin enough to keep your guard up.
And that may be the most useful stance for now. Hope is fine. Hype is expensive.
This article is for educational purposes only and should not be considered medical advice. Always consult a qualified healthcare provider before making decisions about addiction treatment. If you or someone you know is in crisis, call SAMHSA's National Helpline: 1-800-662-4357 (free, confidential, 24/7).