Addiction Care Stigma Starts at Home
Addiction Care Stigma Starts at Home If someone you love is dealing with substance use, the hardest barrier may not be cost, distance, or even denial. It may…
Addiction Care Stigma Starts at Home
If someone you love is dealing with substance use, the hardest barrier may not be cost, distance, or even denial. It may be addiction care stigma. That bias shows up in family conversations, workplace attitudes, and even in healthcare settings. And it matters now because stigma can delay treatment, increase shame, and make relapse more likely.
Boston Medical Center has argued that fighting addiction stigma starts close to home, which tracks with what many clinicians and families see every day. People with substance use disorder often face moral judgment instead of medical care. That framing pushes people away from help. If you want better odds for recovery, safer choices, and more honest conversations, you have to deal with stigma head-on.
What to focus on first
- Addiction care stigma often begins with language, tone, and assumptions inside families.
- Substance use disorder is a medical condition, not a character flaw.
- Shame can keep people from seeking treatment, medication, or harm reduction support.
- Small changes at home can make treatment feel possible instead of punishing.
What is addiction care stigma?
Addiction care stigma is the set of negative beliefs and behaviors aimed at people with substance use disorder and the care they need. It can sound blunt, like calling someone weak or reckless. It can also sound polished, like insisting they just need more discipline.
Look, stigma is not always loud. Sometimes it hides in the quiet stuff. Family members stop trusting a person with any responsibility. Doctors spend less time with them. Employers see risk before they see a worker. That pileup changes outcomes.
When addiction is treated as a moral failure, people often avoid the very care that could keep them alive.
Why addiction care stigma keeps people from treatment
People who expect judgment are less likely to ask for help. That is common sense, but it is also backed by years of public health research on substance use, mental health, and healthcare access. If treatment feels like a courtroom, why would anyone walk in voluntarily?
Stigma can shape each step of care:
- A person hides their use longer.
- Family conflict gets sharper and less productive.
- Primary care visits become incomplete or misleading.
- Treatment starts later, often after a crisis.
- Relapse gets treated as proof of failure instead of a sign that care needs adjusting.
That last point matters. Relapse can happen in many chronic conditions. Addiction treatment is closer to managing asthma or diabetes than passing a one-time test. Families who grasp that tend to respond better under stress.
How stigma shows up inside families
Home is often where beliefs harden fastest. A parent thinks tough love means cutting off every conversation. A spouse monitors every move but refuses to discuss medication for opioid use disorder. A sibling jokes about rehab as if it were a punchline. None of that helps.
Words shape the room.
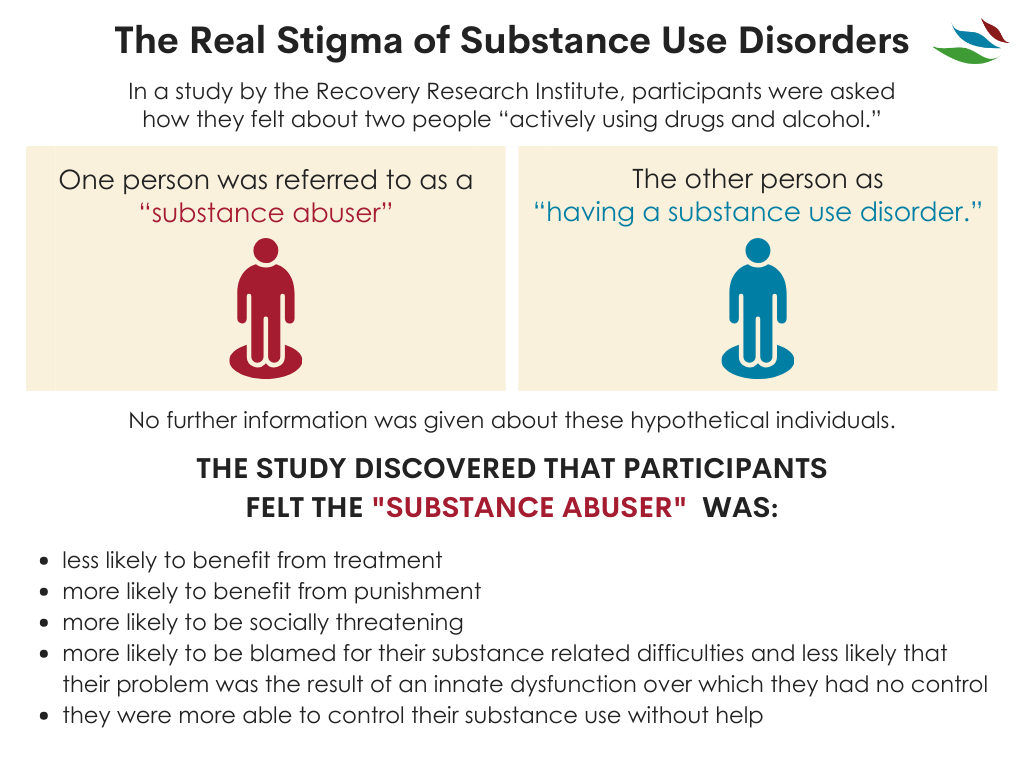
Terms like “addict” or “junkie” reduce a person to a condition. Person-first language, such as “person with substance use disorder,” is more than etiquette. It lowers blame and opens the door to problem-solving. The National Institute on Drug Abuse and other health groups have pushed this shift for years for a reason.
Common signs that stigma is driving the conversation
- You focus on punishment more than safety or treatment.
- You treat medication-assisted treatment as cheating.
- You assume relapse means the person does not care.
- You avoid talking about overdose risk because it feels embarrassing.
- You expect instant trust before any recovery plan is in place.
Honestly, families under strain do not need guilt piled on top. They need a clearer playbook.
What to do at home instead
Think of this like rebuilding a damaged foundation. You do not fix a cracked house with louder yelling. You stabilize the base, then you repair what you can.
1. Change the language first
Drop labels that turn a health issue into an identity. Use direct, neutral language. Ask, “How can we help you get care?” instead of “Why are you doing this to us?” That one shift changes the whole temperature of a conversation.
2. Treat evidence-based care as non-negotiable
Medication for opioid use disorder, counseling, primary care, peer support, and harm reduction all have a place. Not every person needs the same mix, but the goal is practical care, not ideological purity. If a treatment lowers overdose risk and helps someone stay engaged, that counts.
3. Make room for honesty
People are more likely to tell the truth when truth is not punished on sight. That does not mean ignoring harm. It means setting boundaries while still making disclosure safer than secrecy.
4. Learn overdose basics
If opioids are part of the picture, keep naloxone in the home and know how to use it. Talk openly about fentanyl risk. A family that refuses these conversations because they feel uncomfortable is acting like a cook who rejects a fire extinguisher because dinner might turn out fine.
5. Support the person, not the chaos
You can care deeply and still refuse theft, threats, or manipulation. Boundaries matter. But boundaries work best when they are clear, calm, and tied to safety, housing, money, or treatment expectations, not to humiliation.
Addiction care stigma in healthcare is real too
Families are not the only source of stigma. Patients with substance use disorder often report dismissive treatment, shorter visits, or assumptions that every symptom is drug-related. That can be dangerous. Pain gets undertreated. Infections get missed. Trust disappears.
Boston Medical Center has highlighted this problem because health systems shape whether patients return for care. And if the waiting room feels hostile, many will not come back. That is one reason integrated care matters. Primary care, addiction medicine, psychiatry, and social support work better when they are connected.
Questions worth asking a provider
- What treatment options do you offer for substance use disorder?
- Do you provide or refer for medication treatment?
- How do you handle relapse if it happens?
- Can you connect us to counseling, peer support, or family services?
- What harm reduction steps should we take right now?
Why this shift matters for recovery
Stigma isolates people. Recovery depends on connection, structure, and care that people can actually tolerate. A hostile family or shaming clinic can undo progress fast, even when treatment slots are available.
But the reverse is also true. Supportive language, realistic boundaries, medication access, and safer conversations can help a person stay engaged long enough for treatment to work. That is not soft. It is effective.
And effective beats performative every time.
A better next move
If your family has been stuck in blame, start smaller than you think. Change one phrase. Ask one less loaded question. Book one appointment with a provider who treats substance use disorder as healthcare, not as a stain on someone’s character.
The wider culture may take years to catch up. Your home does not have to wait.
This article is for educational purposes only and should not be considered medical advice. Always consult a qualified healthcare provider before making decisions about addiction treatment. If you or someone you know is in crisis, call SAMHSA's National Helpline: 1-800-662-4357 (free, confidential, 24/7).